Standardization: Why the future of medical speech pathology depends on it.
Page 1 of a free guide to help you cut through the clinical chaos (See link at the end of the article to download the whole guide).
Imagine a patient named Arthur. After a mild stroke, Arthur's swallowing was evaluated using traditional, subjective methods. His SLP observed a wet vocal quality, documented his tongue strength as poor using a tongue depressor, and recommended a diet of nectar-thick liquids.
Arthur’s recovery stalled, and he kept returning to the hospital with respiratory issues. Why? Because the ambiguous, non-standardized language essentially failed him. His wet vocal quality was never confirmed with an instrumental swallowing evaluation. His lingual “weakness” was never objectively assessed in terms of kilopascals. And he wouldn’t touch the nectar-thick liquids, which seemed to have a different consistency each time he was served by a different CNA or nurse.
To be frank, nobody really confirmed his deficits or provided an evidence-based approach for getting better. His treatment plan was based on a series of guesses rather than a scientific, evidence-based, objective approach.
I can only hope you are cringing while reading this, as much as I am while writing it.
What’s the answer?
Standardize your practice.
Adopt objective, measurable metrics and abandon the subjectivity that has deeply interwoven itself into how we document and communicate with patients, colleagues, and the entire interdisciplinary team. Instead of guessing and hoping, we are pinpointing and confirming.
Standardization keeps us credible and reproducible, and it keeps us effectively targeting the right deficits with the right approaches.
We want our colleague to see our patient and know how to measure any functional change using the same tools and procedures.
Where are we today?
The truth is, in the medical field, there’s always room for progress when it comes to turning subjectivity into objectivity. Nobody wants a cancer diagnosis to ride on their doctor’s mood or how many more patients they were trying to rush through that day. We want the process to be scientific with mathematical precision.
It’s no different for medical SLPs, and there’s A LOT we can do to make our practice more objective.
The alternative—what many SLPs are still doing today—is steeped in ambiguity. Think about Arthur's initial evaluation. What exactly does "nectar" mean? How do you reliably define "reduced strength?" When we can't translate a clinical finding into something measurable and re-testable, it becomes an unreliable data point, stripping it of its meaning. It’s like saying a cake should be baked at 375 degrees, but then finding out that every single oven’s reading is 50 degrees off.
Then there’s Arthur's wet vocal quality: Are we even able to detect this accurately?
Ask yourself if you can or can’t before reading on. Think you can? Here’s some research that might just prove you wrong.
A 2010 study by Groves-Wright, Boyce, and Kelchner used randomized audio samples of patients speaking during an instrumental swallowing evaluation to answer this question. The results were staggering: Wet vocal quality was accurately identified only 6% of the time.
6%.
It gets worse… Interrater reliability was poor, too—meaning clinicians couldn't even agree on which voices sounded wet and which didn’t.
What should you do instead?
The solution is simple: build a standardized approach relying on objective, consistent findings we can all agree on. Here are three ways to get you started:
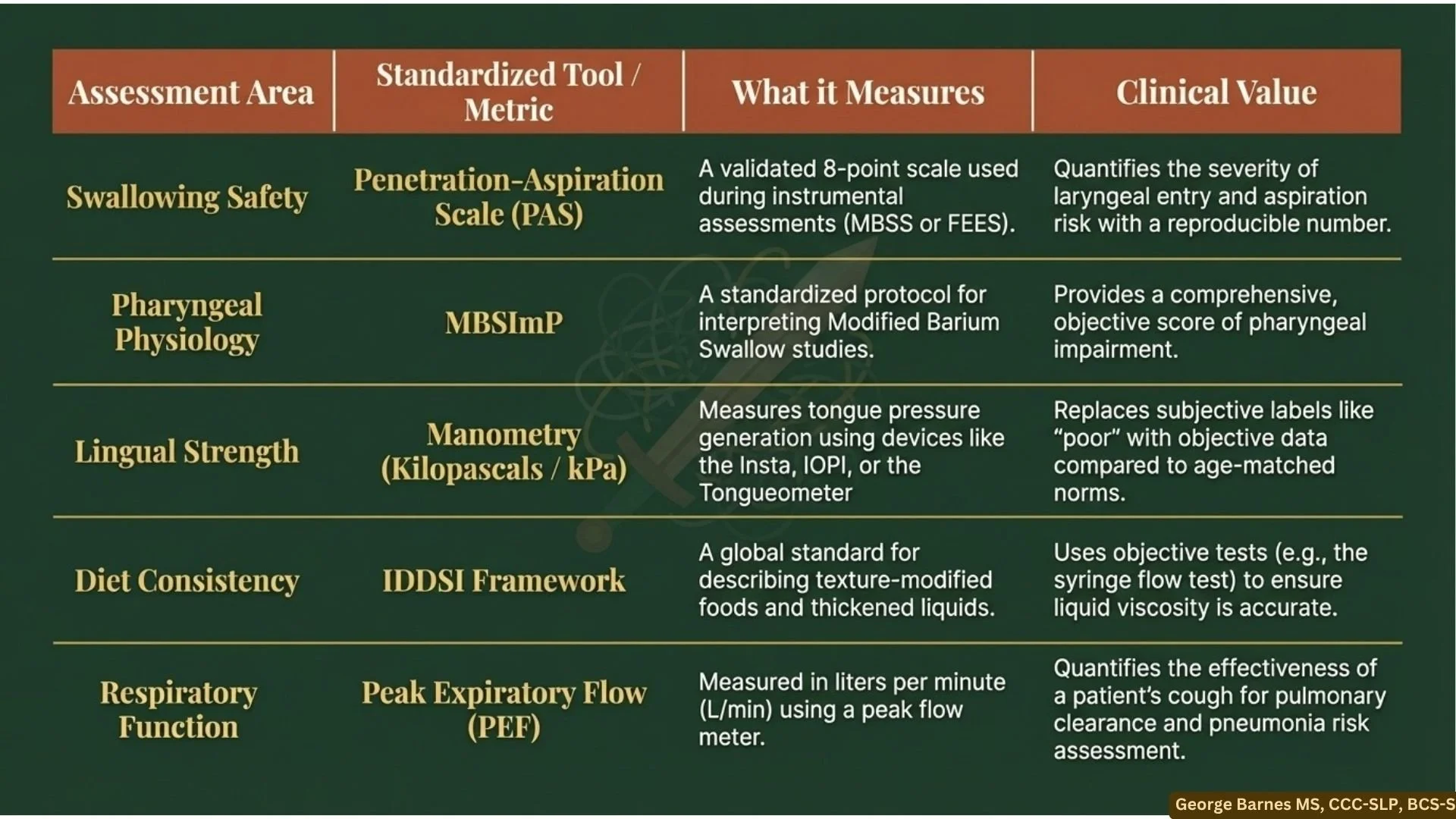
Instead of guessing based on voice quality, conduct an instrumental evaluation and quantify aspiration and penetration using the Penetration-Aspiration Scale (PAS).
Instead of arbitrary, non-standard labels like "nectar thick," we use the IDDSI framework to objectively test liquid viscosity (e.g., using a syringe flow test) and confidently label it "mildly” or “moderately” thick.
Instead of using a tongue depressor and calling lingual strength "poor," we use manometry devices to measure it in exact Kilopascals (kPa) and compare it to age-matched norms.
The best part is that these tools already exist. And they have existed for a very long time.
For example, the Mann Assessment of Swallowing Ability (MASA), a fantastic structured bedside assessment, has been around for over 20 years. Yet, many still don't use it. IDDSI was created over a decade ago, but there is still a good chance facilities aren't implementing it. We also have peak expiratory flow (PEF) meters to measure cough effectiveness, as well as validated questionnaires such as the EAT-10 and SWAL-QOL to track symptom severity and quality of life. Are we all taking advantage of all the tools that are out there?
Bit by bit, incorporating these standardized approaches proves to doctors and patients that our decision-making is rooted in science and research literature. The absolute best way to prove our value is to actually be valuable—by showing tangible, objective, quantifiable improvement.
So, let's look at how Arthur's life changed when he transferred to a facility that had fought for and embraced this standardized approach. His new SLP didn't guess; they used the MASA for a structured bedside evaluation and performed an MBSS, scored with the MBSImP and PAS, to obtain a reproducible, objective score of his pharyngeal impairment and aspiration risk. His diet was better managed using the IDDSI Framework, ensuring his liquid viscosity was perfectly accurate every single time he drank. His tongue strength was measured in Kilopascals, giving him exact, quantifiable targets for his rehabilitation.
Because his progress was tracked with undeniable, objective data, his care team knew exactly when his swallowing had safely improved enough to upgrade his diet. Arthur finally progressed, avoided aspiration pneumonia, and achieved a better quality of life. How? Through standardized, objective science… The foundation of our practice.
Liked this? Click here for a free chart detailing the many ways you can standardize your practice today.