Palliative Care: What can the SLP do when “fixing” the swallow is no longer possible?

Thank you to Irene Gofman Brettman MS, CCC-SLP & Amanda Warren MS, CCC-SLP for sharing their knowledge and helping to edit and approve the contents of this article.
Medical speech-language pathology can feel like a constant race to “fix" things…
But when we step into the world of dementia, palliative care, and comfort measures, the finish line shifts. We are no longer expected to get the patient where they’re going. Instead, our role is to meet them where they are. It’s a shift in mentality that doesn’t always come naturally.
Meet Arthur
Consider a patient like Arthur. Arthur has advanced dementia and has started turning his head away from the spoon during meals. In a traditional rehab mindset, our team members may call this "non-compliance" and worry about his caloric intake or the risk of aspiration.
But if we look through a palliative lens, we see this “non-compliance” as a form of communication. Arthur is speaking to us even though he is non-verbal. He’s saying quite clearly that this bite of pureed beef is not in his care plan. Fair.
By recognizing and appreciating his right to decline food or liquid—and training his family to offer small amounts of his favorite food and drinks—we shift from a battle of wills to a journey of support.
And isn’t that so much nicer? I’d much rather get a patient headed where they’re trying to go rather than convince them to go in the opposite direction.
What’s the difference between palliative care and hospice care?
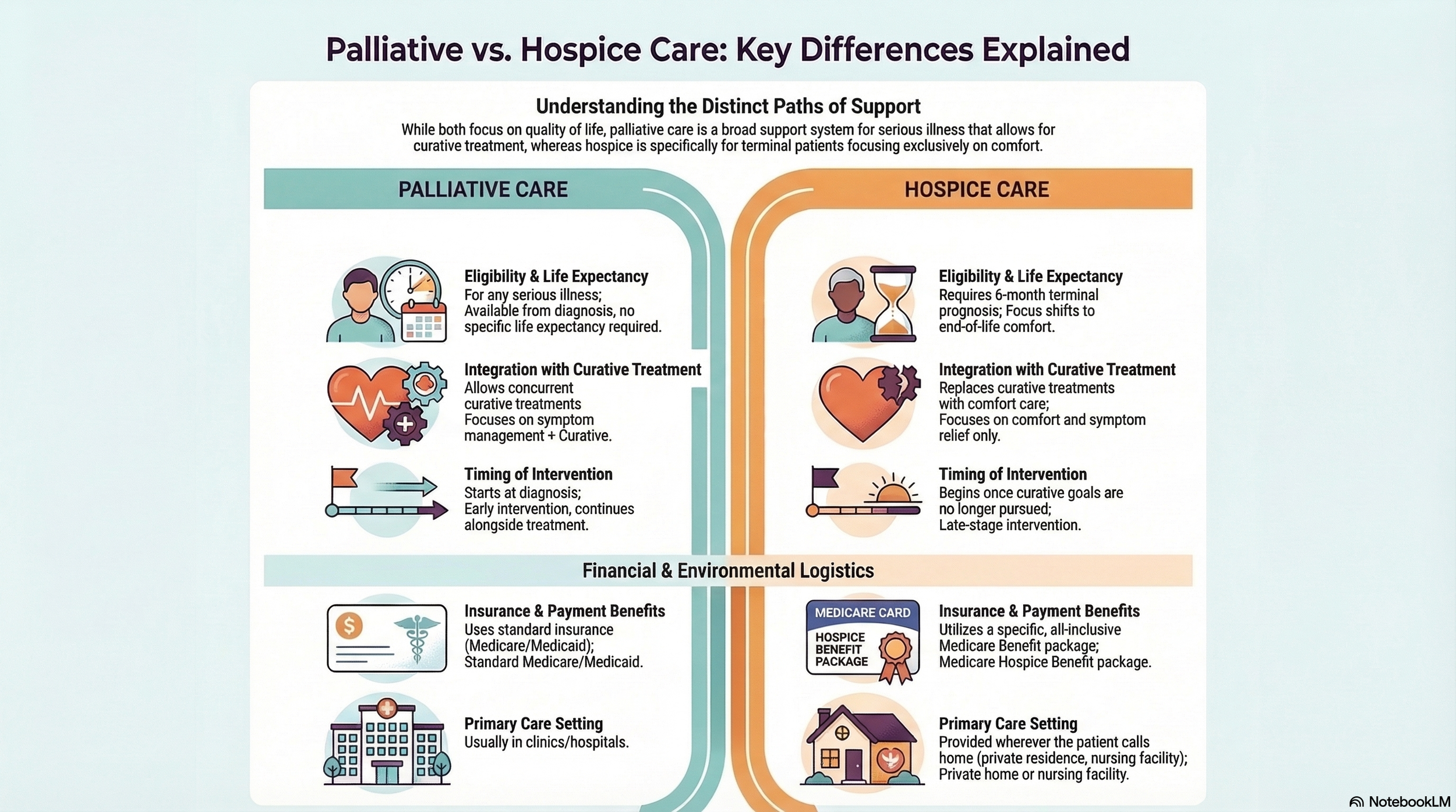
Most people think that palliative care is just another word for hospice. But palliative care is the umbrella. Hospice is only one very specific spoke under it. Palliative care is all about providing a layer of support and symptom relief for anyone with a serious illness. Most people also don’t know that palliative care can start the very day someone is diagnosed, even while they’re still pursuing curative treatments like chemo or surgery. It’s not a death sentence. It’s not giving up. It’s just a little extra help to stay comfortable when your diagnosis has taken much of that away.
Hospice, on the other hand, is a specific insurance benefit package. It’s designed for when the goal shifts entirely away from a cure because life expectancy is measured in months rather than years. Essentially, all hospice is palliative care, but not all palliative care is hospice. Palliative care is the toolbox. Hospice is just one tool among several in that box (i.e., disease management, advance care planning, social and emotional support services, etc.). Understanding this is key because palliative care can offer options that patients and families may not have considered before. And without the guilt of feeling like they are “giving up.”
Below is a chart to help you understand the key differences between palliative and hospice care.
Could palliative care help people live longer?
As you have probably already noticed, there is a great deal of confusion surrounding palliative care. In fact, most people incorrectly believe that palliative care expedites death. Some go as far as to refer to it as the “grim reaper” service. The confusion extends to medical providers, too.
For example, Kavalieratos et al., 2014 found that doctors admit they use hospice and palliative care interchangeably and wouldn’t even know how to get started with a palliative care approach. One doctor said, “I think that the trigger to get [the palliative care service] involved was knowing that my patient was dying and that I didn't have other medical options for them.”
Let’s be clear: palliative care isn't a death sentence. In fact, Temel et al., 2010 showed that patients who get palliative care early in their diagnosis often have a better quality of life, improved mood, and in some cases, even live longer. That’s right, palliative care could help people live longer. There’s a mind shift for you.
Let’s shift gears away from the what and toward the how. How can we add value to patients at the end of life?
Can patients with dementia actually learn?
Despite the myths that are flying around, our patients with dementia absolutely have the ability to learn new information. Memory loss and difficulty retaining new memories are certainly hallmarks of this degenerative disease process, but there’s actually a lot we can do to support patients with dementia in learning information to make their lives easier, safer, and better.
Here’s a simple therapy with a BIG impact:
Spaced retrieval is a technique that assists individuals with dementia in retaining new, functional information. This is achieved by asking them to recall the information over intervals that progressively lengthen. This, with external cues, can create an environment where we aren’t just watching a patient decline, but instead actively supporting independence for as long as possible.
So the next time someone discounts your goals or your plan of care and encourages you to write off your patient with dementia, show them this research and make it clear that there’s still A LOT we can be doing to help these patients.
Care doesn't happen in a vacuum
It happens in a culture. Culture can be summed up in a quick story: Two blue fish swim past a red fish. The red fish says, “Hey, how’s the water today?” The two blue fish continue to swim forward. One turns to the other and says, “What the hell is water?”
It’s hard to describe or even recognize how our own cultural norms and values dictate how and why we do what we do. But we can recognize when others deviate from it. Western medicine clearly puts the patient at the center of the action. They are the customer. Not the daughter, not the son, and especially not the distant friend who asks a thousand questions but is nowhere to be found in the chart. The patient is number one. If someone comes to the store to get a bespoke suit, we wouldn’t ask them what their son’s size is, would we? But that rule doesn’t necessarily apply to healthcare in other cultures.
For example, in some parts of Europe and Asia, the Western standard of disclosing ALL health information directly to the patient can be seen as incredibly rude or even cruel. Families in these cultures often act as a protective shield, preferring to handle the diagnosis and prognosis themselves rather than having a doctor tell the patient directly. No matter how strong a clinician you are, you’re not going to break these cultural barriers anytime soon. Instead of rowing against the current, use your understanding of these norms to determine what’s most important for the patient and how you and their family can support them in their final days (whether or not the patient is fully aware of the time clock).
Assuming everyone thinks or should think the way we do would be missing the point of what our role is in healthcare. When was the last time you convinced a family member to vote for the opposing political party? Never? You’re not alone (If someone has achieved this, give me a call). We don’t have to agree with someone to help them. And that rule should apply no matter what culture we find ourselves in.
What makes a good goal?
Yes, our goals need to be SMART (Specific, Measurable, Attainable, Relevant, and Timely), but they also need to be functional for the patient's stage of life. A goal is only useful if it meets the patient's current needs.
So, how might goals look at an end-stage disease process? Let’s look at a few traditional goals and a few palliative care goals so you can understand the difference:
Traditional Goal: Patient will perform a compensatory chin tuck strategy during 90% of thin liquid bolus trials to eliminate signs of aspiration during a 30-minute feeding session within 4 weeks.
Palliative Goal: Patient will independently utilize a picture menu to select one preferred snack daily for 5 consecutive days to maintain autonomy in care choices by the end of the month.
Traditional Goal: Patient will complete a tongue strengthening protocol for 3 sets of 10 repetitions, 3 times daily, to increase lingual pressure and reduce pharyngeal residue by 50% as measured by a follow-up instrumental exam in 6 weeks.
Palliative Goal: To maintain the joy of social connection, patient will utilize individualized safe swallow strategies to consume 4oz of preferred thin liquid during one family meal daily with zero signs of distress (e.g., coughing or throat clearing) for a period of 2 weeks.
You’re not starving them. You’re helping them.
One of the hardest things for a family to watch is their loved one pushing away a plate, and it’s completely natural for that immediate fear of "starving" to kick in. We often equate food with love and life, so when a patient with advanced dementia stops eating, we worry they are suffering from intense hunger or thirst. But research shows that as the body begins its natural process of shutting down at the end of life, the sensation of hunger actually diminishes. Even more surprising is that the dehydration that occurs in this terminal phase can have a natural analgesic effect, actually increasing comfort rather than causing pain. Understanding that the body has its own way of easing this transition allows us to stop fighting the biology and start focusing on the person: their wants, their needs, and their comfort.
Make Yourself Obsolete
Have you ever wanted more than anything to no longer be needed? Probably not, right? But in palliative care, that’s exactly what we want. Our ultimate goal is to make ourselves obsolete. We do this by becoming master trainers. When we teach a caregiver how to use hand-feeding techniques, make eye contact, use a gentle tone, and go at the patient's pace, we leave a legacy of care that continues long after our discharge summary. Don’t wait. Start the training from day one so you can address barriers, reinforce key insights, and adapt your approach to the patient's evolving needs, while teaching the caregiver to do the same. The greatest accomplishment in palliative care is for a patient’s loved one to say, “Thank you. We have it from here.”
Back to Arthur
Back to Arthur. Instead of a feeding tube and a clinical environment, his family chose a palliative path. He continued to receive medical treatment and therapy, but with a heavy focus on comfort. A feeding tube didn’t fit in that plan of care. He received spaced retrieval therapy to improve his recall of mealtime safety, which made his meals more pleasant and less stressful.
His son was trained on comfort feeding so that Arthur could spend his final weeks tasting his favorite chocolate milk and listening to his favorite jazz records, surrounded by people who understood him best. We didn't "fix" his swallow, but we helped him maintain his dignity until the very end. That is the heart of palliative rehabilitation.
For those interested in delving deeper into this subject, the course "Tackling Palliative Rehabilitation" offered by Northern Speech Services is highly recommended. Please note that this is an independent recommendation, and I receive no financial incentive or sponsorship for promoting this course or article.